Visualizing what it takes to generate a payment in the healthcare sector: the payment use case map

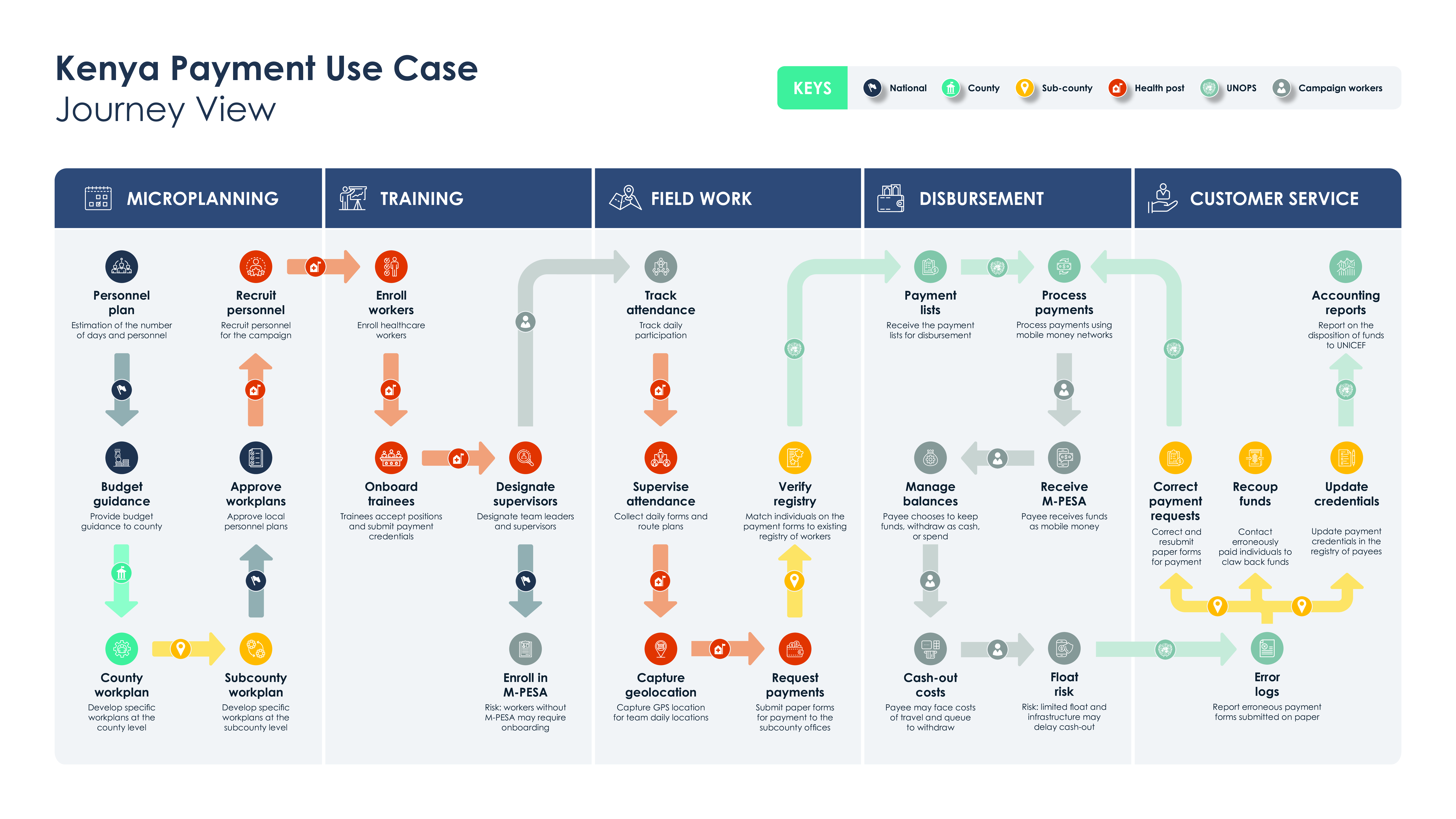
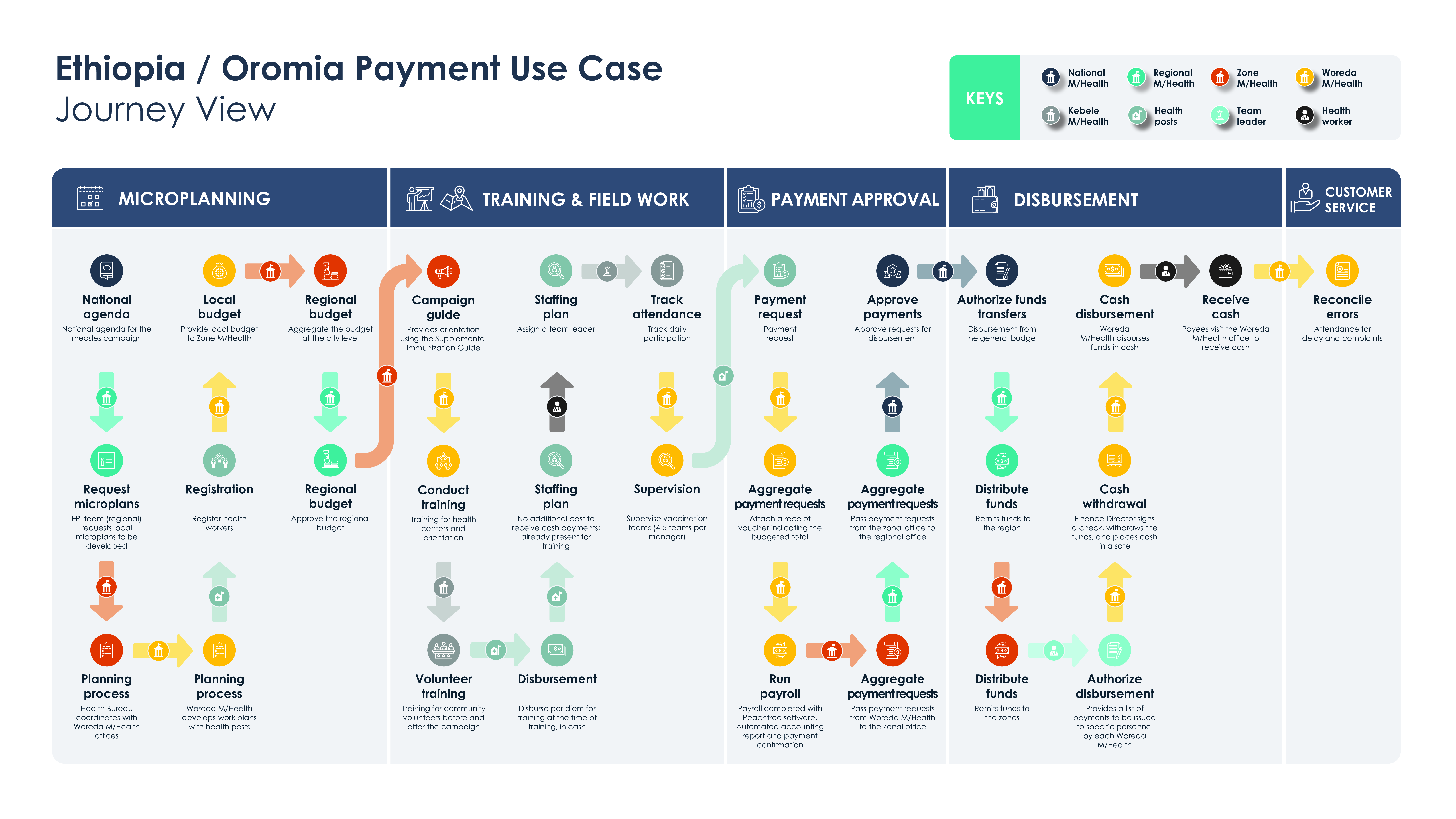
We introduce the research technique of a payment use case map to investigate the benefits of digital payments for frontline healthcare workers. Each payment use case map is a visual map of the steps required to authorize and disburse payments for wages and stipends that support vaccine campaigns (supplemental immunization activities) in Burkina Faso, Ethiopia, Kenya, and Nigeria. These maps detail who does what: the main responsibilities of key stakeholders at the national, regional, and local level. They cover the planning and budgeting phase of the campaign, training and field operations, and finance and administrative processes after fieldwork has largely concluded. They illustrate why local health posts and national health ministries may have different responsibilities in different countries, and what that means for planning the transition to digital payments.
Why aren’t healthcare workers leading the transition to digital payments in more markets? To investigate this question, we studied the institutional setting for healthcare payments in four countries, specifically to support vaccine campaigns (supplemental immunization activities, or SIAs, as they are known in public health). The findings suggest important reasons to accelerate the digital transition and how it would benefit specific stakeholders. This first blog post in a series of three maps the organizations and cost centers involved in payments for vaccine campaigns — in short, who does what, and what it costs.
Digital payments offer some advantages over cash for vaccine campaign workers. Cash is costly and dangerous to distribute. It doesn’t always arrive on time. It is vulnerable to leakage. Whereas digital payments are immediate, direct, and verifiable. The digital transition seems to be beneficial to healthcare ministries that oversee payments, even after accounting for the fees associated with digital payments. To quantify the benefits of the digital transition, it is not sufficient to estimate the costs of cash in transit and the cost of digital payment fees. The cost-benefit analysis should cover all of the administrative and operational changes associated with a transition from cash to digital.
The first product of this research effort was a series of payment use case maps. Building on a methodology used by the Better Than Cash Alliance (see: payment value chains), we created a visual map of the steps required to authorize and disburse payments for vaccine campaigns. These maps detail the main responsibilities of key stakeholders at the national, regional, and local level. They cover the planning and budgeting phase of the campaign, training and field operations, and finance and administrative processes after fieldwork has largely concluded. They illustrate why local health posts and national health ministries may have different responsibilities in different countries, and what that means for planning the transition to digital payments.
The study focuses on five vaccine campaigns in four countries: Burkina Faso, Ethiopia, Kenya, and Nigeria. These countries represent large (Nigeria) and small (Burkina Faso) populations, digital leaders (Kenya) and followers (Ethiopia), and a mix of centralized (Nigeria) and decentralized administrations (Ethiopia again). Moreover, we looked specifically at vaccine campaigns as a case of episodic payments. They have finite operations in geography and time, with a high proportion of temporary or seconded workforce, and a mix of wages and stipends for operational expenses such as petrol and lodging.
These countries were selected because they each had a recent and sizable vaccine campaign for measles since 2018. Measles catch-up campaigns in particular have broad geographic coverage within the country and a similar focus on children, primarily under 5 years of age, where the intent is to ensure national coverage rather than in response to a specific epidemic. Burkina Faso distributed payments principally in cash. Two regions of Ethiopia used different methods, bank transfers and cash. Nigeria distributed funds by bank transfer. And in Kenya, two successive campaigns (2016 and 2021) used different methods, cash and then mobile money.
The payment use case maps synthesize what we learned about budgeting and payment administration from dozens of interviews with staff at all levels: immunologists, public health experts, finance and administration leaders, local government officials, health post leaders, frontline healthcare workers, donors, and regional bodies that support finance and operations. This set of activities, organized as they are, provides one framework for analyzing the cost of payment-related activities in staff time and budget, which we did using original financial records. Finally, we modeled the costs incurred by recipients to transform balances — either from cash into mobile money, for security, or by cashing out mobile money. We modeled those costs based on current M-PESA tariffs and survey evidence on user behavior.
The result is a map of activities with some common patterns, such as the five phases from budgeting to disbursement, and important differences between countries.
National healthcare systems can be centralized or decentralized in two different aspects: first, finance and administration; and second, personnel and operations. In countries with centralized finance and administration, the national government may directly disburse payments to frontline healthcare workers. Decentralized finance and administration means that more of the payment processes and financial controls are devolved to a local level. Decentralization of finance allows for somewhat more flexibility at the local level in replacing cash with digital payments; whereas centralization allows for more national control over payment methods.
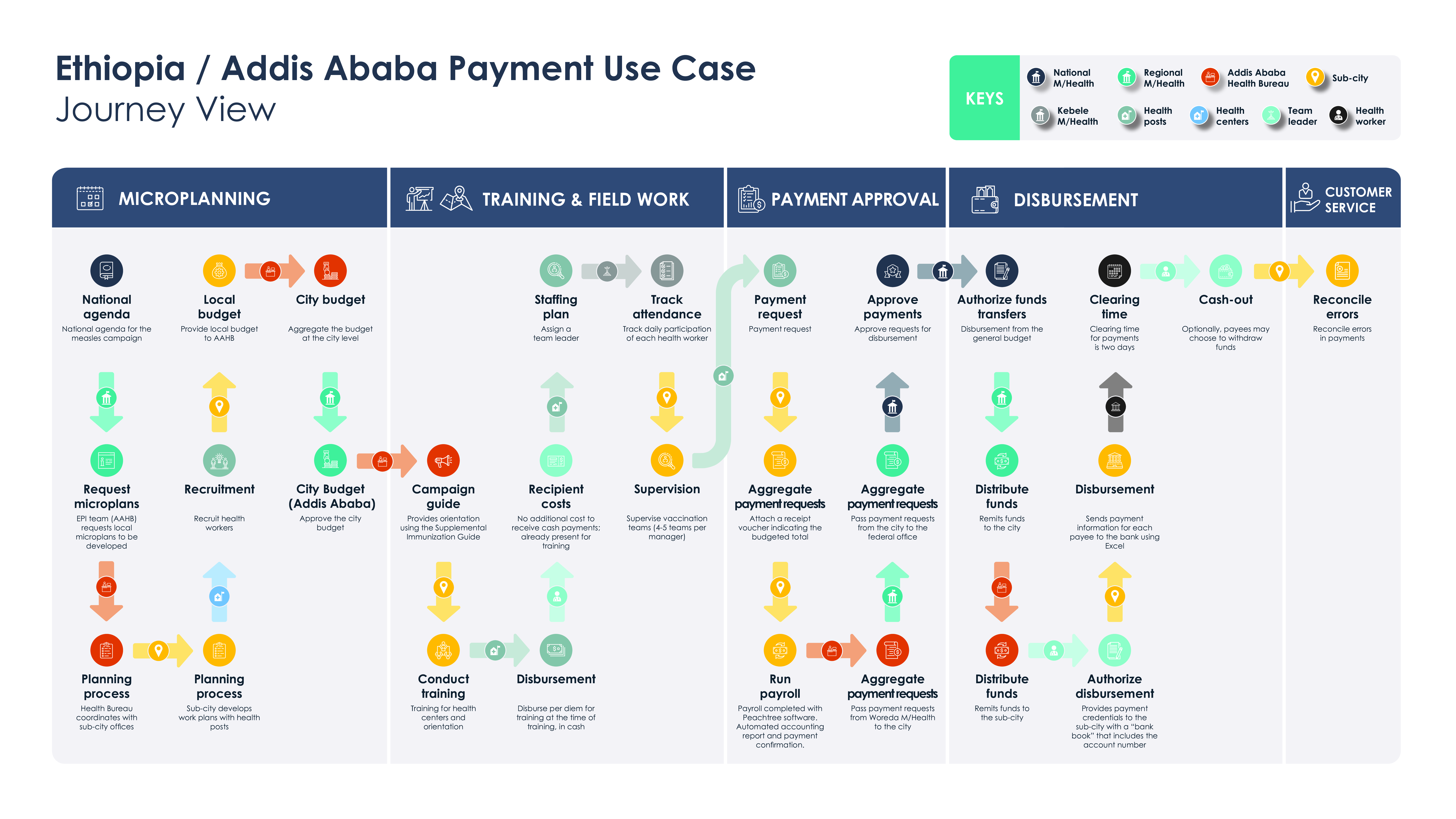
Personnel and operations may also be centralized or decentralized. In a centralized operational context, local healthcare bodies may submit detailed plans for personnel and operations in accordance with national policies and procedures. Decentralized operational context means that regional governments may conduct largely separate campaigns with broadly coordinated oversight and financing mechanisms. Ethiopia was so decentralized that we created separate payment use case maps for two of its regions.
The payment maps are a critical tool for understanding what processes are implicated in a transition to digital payments, and who are the stakeholders that must be involved. These are highly diverse countries, and there is no silver bullet for advancing the transition to digital payments. Yet the potential advantages of digital payments for improving the speed and accuracy of these payments are too great to ignore. Armed with these maps, one can develop effective plans to manage the digital transition with local buy-in and realize important benefits for efficiency and risk management.
We invite you to read the full report and consider how to apply the payment use case map methodology in service of campaign effectiveness.
This work was made possible thanks to the generous support of the Bill & Melinda Gates Foundation. We are grateful for the participation of the Gates Foundation country staff in Burkina Faso, Ethiopia, and Nigeria; Gates Foundation healthcare effectiveness teams; as well as key personnel from the Kenya Ministry of Health, the Nigeria Ministry of Health, regional and local health officials in the Addis Ababa and Oromia regions of Ethiopia; and United Nations Office for Project Services (UNOPS). We also thank Clearskies Technology, our field research partner in Ethiopia.
Return to the executive summary
This material was prepared for the Bill & Melinda Gates Foundation. The findings and conclusions contained within are those of the authors and do not necessarily reflect the positions or policies of the Bill & Melinda Gates Foundation.


